Background Microbiology and Virulence
Clostridium difficile (C. diff) is a fascinating bug. It is a Gram-positive, spore-forming, toxin-producing, obligate anaerobe that, like other organisms in the Clostridium genus (e.g. C. botulinum- causative agent of botulism, C. tetani- causative agent of tetanus), wreak havoc on the human body with their toxins. C. diff's toxins most often cause diarrhea but can also cause more serious conditions such as pseudomembranous colitis. Here are a few images of the damage that can be done:
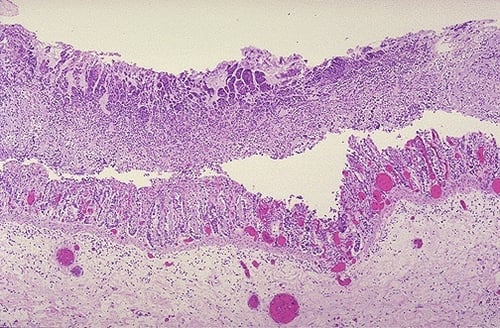
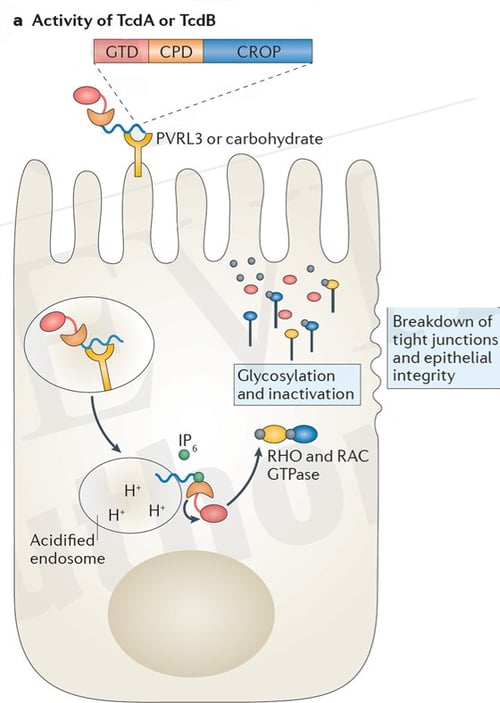
The damage seen above, as I mentioned, is caused directly by the action of C. difficile's two toxins, TcdA and TcdB. These are (relatively) massive toxins, and in fact, some of the largest toxins known. The toxins get taken up by the host cells via endocytosis and modify host enzymes that, in turn, disrupt the cellular architecture eventually causing cellular death and a breakdown of tight junctions and epithelial integrity. A great schematic of the toxin activity is below (source from Abt, et al. in Nature Reviews Microbiology here).
It has classically been thought that most patients became infected via hospital acquired infections. The use of wide-spectrum antibiotics would then obliterate the individual's microbiota, allowing C. difficile to colonize and flourish. The literature suggests, though, that the percent of hospital-acquired infections may have been overestimated in the past, suggesting that asymptomatic carriers and community-acquired infections play a bigger role than previously thought. There's an interesting article in the New England Journal of Medicine on that here by Eyre, et al. Regardless of how a person gets infected or colonized, the disruption of the host's microbiota, most notably from the use of wide-spectrum antibiotics, can allow the organism to colonize, flourish, and cause issues.
EHR Optimization - Ordering C. difficile Testing in Epic/Beaker
Age-Based RecommendationsAs I mentioned above, asymptomatic carriage is possible and in fact, extremely common for children under the age of 1. So children with diarrhea could test positive, but simply be an asymptomatic carrier of C. difficile. Given this, the IDSA strongly recommends against routine C. diff testing in infants. To help ensure appropriate use, you should put this recommendation into Epic to help guide clinicians. You can simply build out an age-based BPA that alerts the ordering clinician that this testing is not recommended for this patient population. The IDSA weakly recommends against testing in patients aged 1 to 2, unless other causes have been excluded. This too could be a BPA that requires the clinician to confirm other causes have been ruled out prior to ordering. In both cases, you could link the clinician to the IDSA guidelines or your hospital's infectious disease documentation on C. diff.
Patient on Laxatives
In addition to the age-based criteria, the IDSA also recommends against C. diff testing if other underlying conditions/causes haven't already been ruled out. One of these is recent laxative use. This, too, could be built by using another BPA that looks through a patient's medications and looks to see if they have taken any laxatives.
Other Underlying Conditions or Causes
The IDSA also lists other conditions that should be considered prior to testing for C. diff, but they don't entirely recommend against testing if the patient has/meets them. These conditions include patients with IBD, patients with a feeding tube, or patients undergoing intensive chemotherapy. These are less black and white as patients with IBD or a feeding tube have actually been shown to be more at risk for C. diff infections than other cohorts of the population (source in the Annals of Internal Medicine). You can run these by your infection control and epidemiology folks to see if they'd like to build anything for these. The good news is that it is possible with Epic. The power of Epic is that all of a patient's medical information is stored in one system. That makes it possible to look to a patients problem list, medications, treatment plans, age, and medical history to help guide ordering. Use Epic to its fullest extent to eliminate unadvised testing, reduce costs, and improve care.
EHR Optimization - Resulting and Viewing Results in Epic/Beaker
The IDSA recommends a multi-step algorithm for C. diff testing as opposed to solely performing a PCR test. The most common paradigm I have seen (which follows IDSA recommendations) first tests (simultaneously) for GDH and the toxins via immunoassay. If both the GDH and toxins are negative, then the patient is considered negative for C. diff. If both are positive, the patient is considered positive for C. diff. If the two results are discordant (e.g. GDH+, Toxin- or GDH-, Toxin+) PCR testing is recommended for confirmation. The final result, then, is really based on the result entered for the three components (GDH, Toxin, & PCR). To simplify resulting for the tech and the subsequent digestion of results by the clinician, make this one test in Beaker with 4 components. The test would look something like this: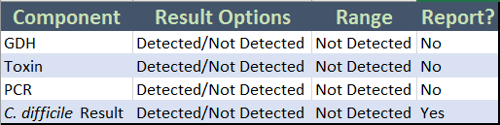
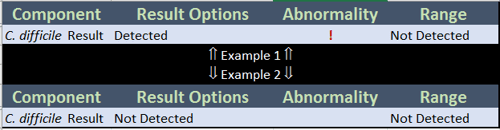
Note that *only* the last component, a somewhat generic "C. difficile Result", will report to the chart. This makes it easy for a clinician to interpret the results with ease. Imagine the alternative, where we report each of these to the chart. Two confusing examples of what that would look like are below:
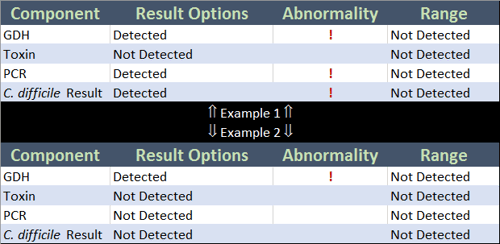
That's confusing. And requires the physician to interpret the results instead of letting Epic do that work for them. Compare the above to the beautiful simplicity of one component in the two examples below:
That is far easier to read and eliminates any potential confusion.
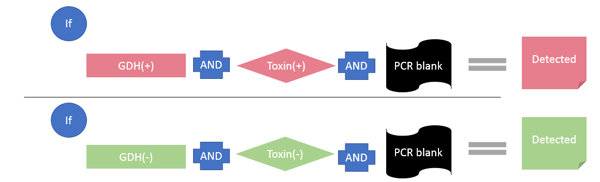
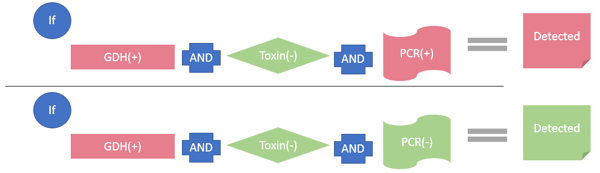
Importantly, we can make the workflow for the techs in the lab easy too. The main "C. difficile Result" component does *not* have results entered by an instrument or the tech - it uses rules based on the results entered on the GDH, Toxin, and PCR components and one generic equation to automatically populate the final result. Equations aren't *just* used for numeric components - you can use them for category-based components too, in conjunction with rules! You would build 6 rules to accommodate each combination of results. Each rule would be placed on the component, with the generic equation on each line, and the result that should be returned for each. If you have any trouble with this build, just get in touch with me and we can chat. I cannot post screenshots of the build here so as to respect Epic's IP, but will happily walk you through the build if you're having any issues! The 6 rules you would build would have the following logic:
That's it! The result will automatically calculate based on the results of the GDH, Toxin, and PCR components automatically. It will be the only component that reports, eliminating possible confusion. Should you have any questions about the above, just get in touch!