In this post, we outline the current guidelines from the Infectious Disease Society of America (IDSA) for Group A Streptococcal (GAS) pharyngitis testing and discuss how you can implement them in your LIS. This EHR/LIS optimization should only require a few minutes of build.
Group A Streptococcal Pharyngitis Testing Guidelines
Rapid strep tests, while being very specific, have variable sensitivities ranging from 70% - 90%. (Gerber & Shulman, 2004; Tanz et al., 2009). Given that, many labs across the US automatically reflex a throat culture following a negative rapid antigen detection test (RADT) to protect against any false negatives.
While the throat culture is undoubtedly the gold standard for testing, should all negative RADTs reflex a throat culture? Not necessarily, according to guidelines from Infectious Disease Society of America (Shulman et al., 2012).
In the guidelines, the authors state:
"Routine use of back-up throat cultures for those with a negative RADT is not necessary for adults in usual circumstances, because of the low incidence of GAS pharyngitis in adults and the risk of subsequent acute rheumatic fever is generally exceptionally low in adults with acute pharyngitis (strong, moderate)."
" In children and adolescents, negative RADT tests should be backed up by a throat culture (strong, high)."
Looking to one of the preeminent reference labs in the nation, ARUP, we see that they follow this guideline exactly (Fisher, 2022).
So how can we make these recommendations a reality in your LIS? Fortunately, doing so should be quite simple.
EHR Optimization for GAS Pharyngitis Testing
Building this out in your own EHR/LIS should be possible with some very simple rule logic that states:
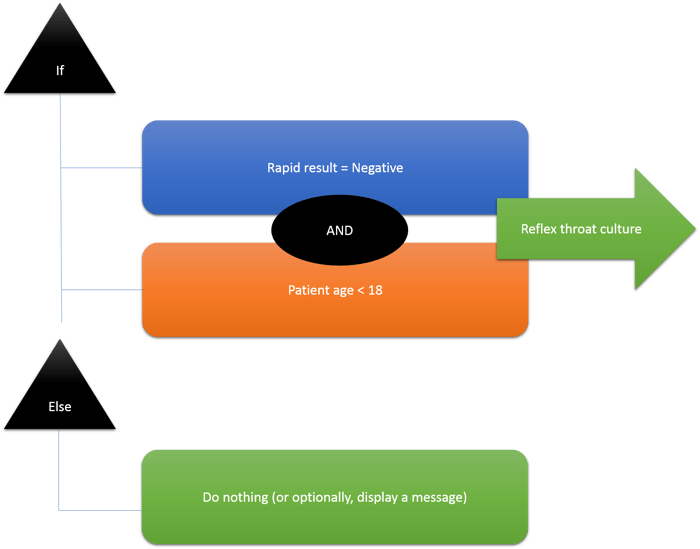
Though it depends on your LIS, you would likely accomplish the above with two rules. The first rule would look to the negative result AND the patient's age. The second rule would simply be NOT equal the same logic. If your rule engine allows custom logic, you can simply duplicate your first rule and say "NOT (criteria 1(result) AND criteria 2(age))" in the custom logic. You'd then plug these rules into your LIS's reflex actions on the rapid strep test. The first rule will trigger the throat culture reflex and the second, which is notably optional, can trigger a display message alerting techs that even though a reflex didn't fire, the system is behaving as it should. The message could state something similar to the effect of, "Throat culture reflexes are not recommended for this patient population."
To further expand on this build, one could add an order-specific question to the rapid strep test procedure that asks the ordering provider if they would like to automatically reflex a throat culture for any patient populations that might require it, overriding the recommendations. The guidelines indicate that there are certain scenarios where this would be acceptable.
One could, of course, create a number of questions with all of the possible reasons that a reflex would be desired, but one catch-all question would likely suffice to minimize order question fatigue for physicians. If pursuing this option, one would simply have to adjust their rule logic to state:
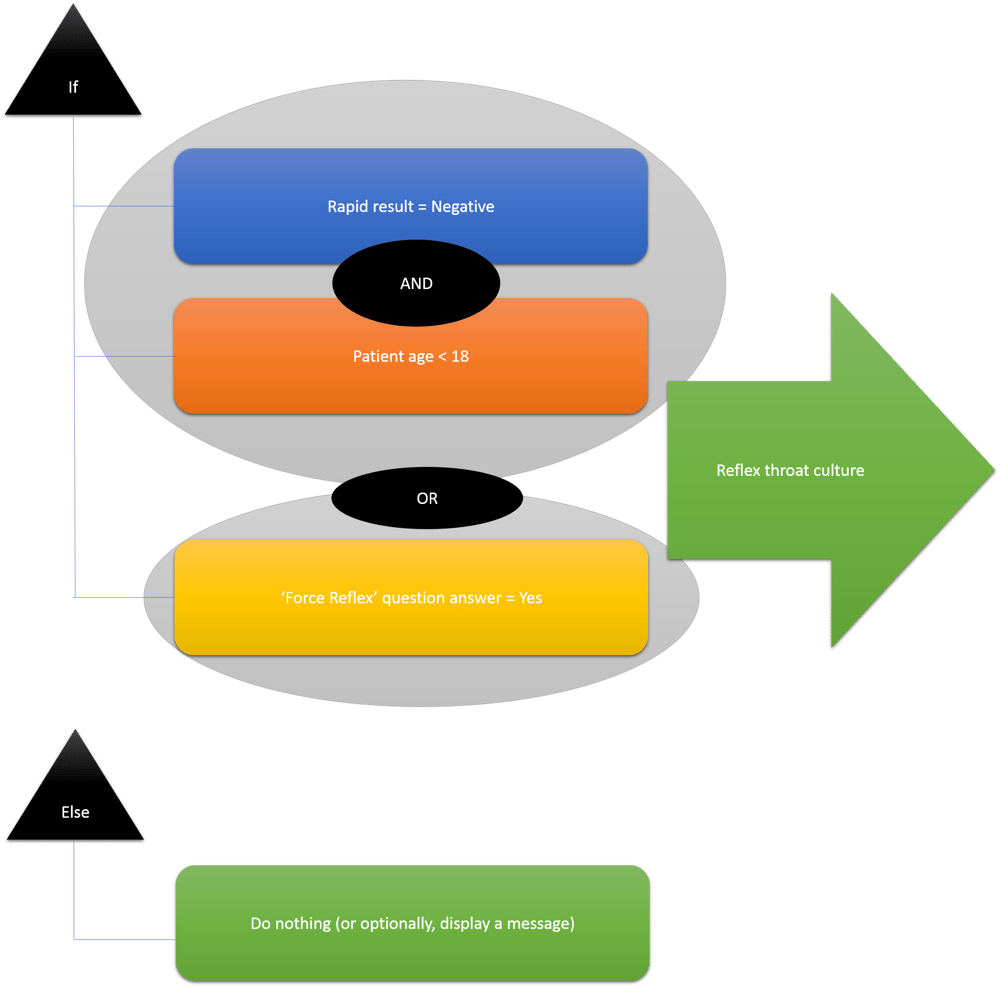
This new logic simply has the original AND conditions with an added OR condition that looks to the response to the order-specific question.
If implementing the question, it would be wise to run reports after a month or so to see if the question is being abused. If it is, you may want to consider defaulting the response to the question to "No", adding additional help text that explains the recommendation a bit more, or reach out to clinicians individually.
What do you think about the suggestions above? Let us know in the comments section below. Have any questions about the build? Feel free to reach out to me and we can discuss.
References
Fisher, M.A. (2022, March). Group A Streptococcal disease - strep throat. ARUP Laboratories. https://arupconsult.com/content/streptococcal-disease-group
Gerber, M.A. & Shulman, S.T. (2004). Rapid diagnosis of pharyngitis caused by group A streptococci. Clinical Microbiology Reviews, 17(3), 571–580. https://doi.org/10.1128/CMR.17.3.571-580.2004
Shulman, S. T., Bisno, A. L., Clegg, H. W., Gerber, M. A., Kaplan, E. L., Lee, G., Martin, J. M., Van Beneden, C., & Infectious Diseases Society of America (2012). Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clinical Infectious Diseases, 55(10), e86–e102. https://doi.org/10.1093/cid/cis629
Tanz, R. R., Gerber, M. A., Kabat, W., Rippe, J., Seshadri, R., & Shulman, S. T. (2009). Performance of a rapid antigen-detection test and throat culture in community pediatric offices: implications for management of pharyngitis. Pediatrics, 123(2), 437–444. https://doi.org/10.1542/peds.2008-0488